 |
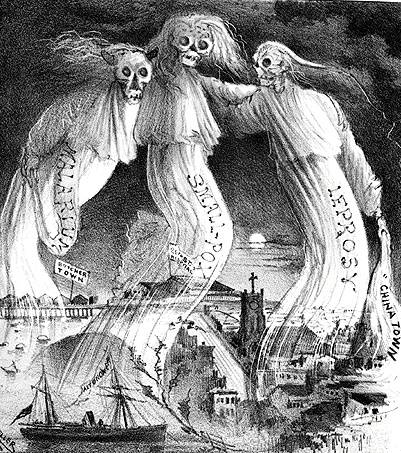
| Cartoon from The Wasp of May 26, 1882, promoting the then-common racist myth that diseases were rampant in Chinatown. |
I am not back.
No time, but I had to post this.
Racism and infectious diseases...today Ebola, yesterday and tomorrow something else. Listen to white supremacist on the net and on the radio and you will get sick to your stomach and want to punch someone out.
The following from Jezebel is a bit more refined, but right on target.
From Miasma to Ebola: The History of Racist Moral Panic Over Disease


On October 1st, the New York Times published a photograph of a four-year-old girl in Sierra Leone. In the photograph, the anonymous little girl lies on a floor covered with urine and vomit, one arm tucked underneath her head, the other wrapped around her small stomach. Her eyes are glassy, returning the photographer's gaze. The photograph is tightly focused on her figure, but in the background the viewer can make out crude vials to catch bodily fluids and an out-of-focus corpse awaiting disposal.
The photograph, by Samuel Aranda, accompanied a story headlined "A Hospital From Hell, in a City Swamped by Ebola." Within it, the Times reporter verbally re-paints this hellish landscape where four-year-olds lie "on the floor in urine, motionless, bleeding from her mouth, her eyes open." Where she will probably die amidst "pools of patients' bodily fluids," "foul-smelling hospital wards," "pools of infectious waste," all overseen by an undertrained medical staff "wearing merely bluejeans" and "not wearing gloves."
EXPAND

Aranda's photograph is in stark contrast to the images of white Ebola patients that have emerged from the United States and Spain. In these images the patient, and their doctors, are almost completely hidden; wrapped in hazmat suits and shrouded from public view, their identities are protected. The suffering is invisible, as is the sense of stench produced by bodily fluids: these photographs are meant to reassure Westerners that sanitation will protect us, that contagion is contained.
Pernicious undertones lurk in these parallel representations of Ebola, metaphors that encode histories of nationalism and narratives of disease. African illness is represented as a suffering child, debased in its own disease-ridden waste; like the continent, it is infantile, dirty and primitive. Yet when the same disease is graphed onto the bodies of Americans and Europeans, it morphs into a heroic narrative: one of bold doctors and priests struck down, of experimental serums, of hazmat suits and the mastery of modern technology over contaminating, foreign disease. These parallel representations work on a series of simple, historic dualisms: black and white, good and evil, clean and unclean.
The Western medical discourse on Africa has never been particularly subtle: the continent is often depicted as an undivided repository of degeneration. Comparing the representations of disease in Africa and in the West, you can hear the whispers of an underlying moral panic: a sense that Africa, and its bodies, are uncontainable. The discussion around Ebola has already evoked—almost entirely from Tea Party Republicans—the explicit idea that American borders are too porous and that all manners of perceived primitiveness might infect the West.
And indeed, with the history of American and European panic over regulating foreign disease comes a history of regulating the perception of filth from beyond our borders, a history of policing non-white bodies that have signified some unclean toxicity.
If the history of modernity can, as Dominique Laporte suggests in his genealogical meditationHistory of Shit, be written as a triumph of cleanliness over bodily refuse, then so too could the European colonization of Africa and India. The sanitary crusade of the nineteenth century is central to the violent project of empire. Western medicine, with its emphasis on personal hygiene, functioned (and in some arenas still functions) as colonialism's benevolent cover—an acknowledgment that, while empire was about profit at all costs, that it could also conceal this motive slightly by concerning itself with bettering the health of debased bodies.
The bureaucratic annals of colonialism are filled with reports on the unsanitary conditions of life and unhygienic practices of natives. Dr. Thomas R. Marshall, an American in the Philippines,wrote of the "promiscuous defecation" of the "Filipino people." An 1882 British report, "Indian Habits," observed that, "The people of India seem to be very much the condition of children. They must be made clean by compulsion until they arrive at that degree of moral education when dirt shall become hateful to them, and then they will keep themselves clean for their own sakes." Dirtiness and defecation indicated their primitiveness and savagery; it reaffirmed the white body's privileged position and claim to moral and medical modernity.
This intense focus on hygiene emerged from an old medical doctrine known as miasma. According to the miasma theory, illness was the direct result of the polluting emanations of filth: sewer gas, garbage fumes and stenches that permeated air and water, creating disease in the process. Filth, however, had many incarnations. It could be literal, or also a catch-all metaphorical designation for anything that made people uncomfortable about race, gender and sexuality. (This idea underpins phrases still in use today, for example: a "dirty whore").
So, the medical mission of hygiene was simultaneously a moral and medical imperative. And it was this fervent belief in miasmas that led to colonial administrations deeply interested in the bodily fluids of bodies of color; as Lord Wellesley, the British governor of India, briefly noted in an 1803 report, "Indians defecate everywhere."
But if colonial governments exercised concern over what they believed to be the contaminated cultures of native populations, it was more likely the result of panic over the health of their own officials and soldiers. "The white man's grave," as one nineteenth-century British colonist called Sierra Leone, was a dangerous trap of foreign disease, carried by the contagious peoples who inhabited valuable land. Their culture, like their natural resources, must be conquered. Who better to do that then scientifically advanced westerners who valued cleanliness and life?
Miasma theory proved a powerful science through which to construct "the African" or "the Indian." Long after its late-nineteenth-century demise and subsequent replacement with an epidemiological understanding of contagion, the metaphors it produced endured. The move from miasma theories to germ theories simply added pathological depth to older social resentments. Minorities might look clean: but who knew what invisible, contagious threats lurked within?
These stereotypes showed up everywhere. Take, for example, Victorian soap advertisements: ordinary markers of domesticity that, according to feminist scholar Anne McClintock, "persuasively mediated the Victorian poetics of racial hygiene and imperial progress." In a Pears' Soap advertisement from around 1882, race is linked to dirtiness and ignorance: blacks could become clean (here, actually, white) if they just bathed; they barely know how to clean themselves; they need a white man to teach them cleanliness, civilization, culture, etc.
EXPAND1

Such metaphors proved successful for Pears' Soap, and the company returned to triumphant colonial imagery time and time again. In another ad from the 1890s, a naval commander (likely a stand-in for Admiral George Dewey) is shown washing his hands; he is flanked by ships that import soap and a missionary anointing his dirty, savage subject with hygiene. Underneath the images, the text reads "The first step toward lightening The White Man's Burden is through teaching the virtues of cleanliness."
But if disease was the result of a certain kind of self-imposed debasement—of a choice to resist modernity—then the moral meaning of dirt was flexible. It could be external, a black body in need of hygienic instruction, but it could also be internal, the naturally occurring state of the nonwestern body. Miasma theory gave way to eugenics; filth was biologically determined, inside and out.
If filth provided European imperialism with a set of legible metaphors about disease and race, then it also gave a newly-forming United States racial principles on which to build a national identity. With institutionalized slavery and a relatively open immigration policy, America, more so than Europe, needed those metaphors to preserve the cultural and moral superiority of particular kind of whiteness (a Teutonic Northern European whiteness). In the late-nineteenth and early-twentieth centuries contagious disease was associated with new immigrant groups who were perceived as harbingers of death.
EXPAND

Nativist groups warned the public of disease that would infect the nation's growing urban areas, rationalizing their prejudice with arguments about public health. In the 1830s, poor Irish were said to bring cholera; at the turn of the century, tuberculosis was dubbed the "tailors' disease" and associated with the Jewish population; Italians for decades were seen as bearers of polio.
To protect against immigrant germs, the United States passed the Immigration Act of 1891, an act that excluded those with "criminal records, polygamist, and prostitutes," as well as those with "loathsome or contagious disease." The Immigration Act made clear that the immigrant carried the filth of both moral degradation and disease. The definition of "loathsome and contagious disease" was flexible and ever-changing, including everything from transmissible disease to insanity, senility, varicose veins, and poor eyesight.
The truth, of course, was that immigrants groups were as healthy as acceptably white Americans.According to contemporary legal scholars, less than three percent of the total number of immigrants seeking entry were rejected for medical reasons; the vast majority of those excluded were Chinese who, unlike their white counterparts, could be rejected for ringworm and "the appearance of mongolism." But yet, despite these facts, white Americans still clamored to close the borders entirely. An 1888 federal report calling for even more immigration restriction warned of the "sewage of vice and crime and physical weakness" that washed ashore from Europe and the "nameless abominations" coming from Asia.
EXPAND2

The language of the 1888 report is similar to the current, persistent calls to close our borders. Both rely on the intertwining metaphors of illness and filth. This, of course, is how the metaphor of disease works. Susan Sontag has written of the hierarchy of disease, of death in a western context. She notes that there are brave and beautiful ways to die, diseases that afflict and kill, yet reveal a beautiful, meaningful self. And the diseased body of white Europeans, particularly the wealthy, is rarely depicted filthy or debased. Rather, that body becomes the source of poetic meaning; think of Henry James's The Wings of the Dove (1902) or Thomas Mann's The Magic Mountain (1927) a novel that describes disease as "nothing but a disguised manifestation of power of love; and all disease is only love transformed."
Perhaps nowhere was the power of a disease metaphor more evident than in San Francisco in 1900. When a Chinese immigrant was found dead in the basement of a Chinatown hotel, rumors spread immediately that he had died of the plague. Before the diagnosis was confirmed, the mayor quarantined Chinatown, preventing anyone of Asian origin from leaving the district while allowing whites to move around freely. Once the diagnosis was confirmed, the city's white residents panicked. The Board of Health demanded the entire district be doused in lye and bichloride of mercury, that clothes and furniture be burned, that every person of Asian descent be vaccinated with something called Haffkine's serum, which had not yet been approved for human use. Newspapers called for Chinatown to be emptied of its residents and burned to the ground.
The measure the city took were in direct opposition to those recommended by health officials. Quarantining an entire population and dousing them with household cleaners made the outbreak worse. The outbreak of plague ended when state health officials stepped in, but the panic served its purpose: it reaffirmed old suspicions that Chinese immigrants were dangerous, and that their foreign lifestyle could easily soil San Francisco's urban modernity.
The plague broke on again in San Francisco, after the 1906 earthquake, but this time it wasn't in Chinatown; it emerged from an overwhelmingly white city district. There was no quarantine, no dousing of the city with lye. Rather, the city spent two million dollars to provide free and sophisticated medical care, and the death toll was much smaller.
Returning to the four-year old Ebola patient in the New York Times: The photograph of a dying little girl is simultaneously a site of sympathy and a powerful reminder of the contagion she carries. As she dies from a vicious, seemingly unstoppable disease, the photograph is meant simultaneously to warn and console. Look at this cesspool, these unsanitary conditions; she is foreign, Ebola is foreign. This scene is by no measure the only scene of healthcare in African countries, but it is often the only scene we see.
This underlying sense of foreignness underlies the way we see Ebola in the United States.Newsweek repeated these ugly stereotypes in an August cover story that conspiratorially suggested that illegally imported African "bushmeat" could carry Ebola into our borders (a story that's been thoroughly debunked).
EXPAND

And when the Centers for Disease Control and Prevention confirmed that Ebola had crossedinto the United States, carried on the body of a black man from Liberia, the threat of infection was suddenly perceived as quite real. Rumors flew that Ebola had reached Idaho, then Miami, that the disease was airborne, and that a sick passenger on a flight to New Jersey was infected. Television and radio host quizzed CDC physicians about the likelihood of infection ("little to none," they seem to answer again and again), asked again about the safety of our too-porous borders, demanding that our government outline a plan of action to ward off infectious, black bodies.
Thomas Duncan, that Ebola patient, is now dead. He sought treatment five days after returning to the US, telling the hospital that he had traveled to Liberia and was experiencing a fever and abdominal pain. With no insurance, he was turned away. A Washington Post story reports that some people close to him feel that he was "not properly treated because he was not American."
"He is a Liberian man," Massa Lloyd, a close friend of Troh, said Wednesday. "The family feels he wasn't getting the right treatment because he was an African man. They feel America is fighting only for the white man, not the black man."
The onset of epidemic disease has always incited prejudice, permitting the stereotyping of foreigners, of people of color, as inherently closer to disease: more deserving of death from it. The "always them, never us" conception of Ebola is a major factor in the lack of a vaccine, which the NIH has been researching, with dwindling funding, since 2001. The new presence of Ebola in the US may change the way we approach the virus, but maybe not; maybe it will always seem too foreign for us to handle it like the global and communal problem that it is; maybe, disastrously, this outbreak of Ebola will be no different than before.
Stassa Edwards is a freelance writer and editor.
Image by Jim Cooke, source photo via Getty.
No comments:
Post a Comment